


Published on Nov 30, 2023
Homo sapiens are born with Spinal Cord which is widely known as the backbone of the body; the spinal cord is divided into a) Cervical vertebrae b) Thoracic vertebrae c) Lumbar vertebrae and d) Sacral vertebrae, overall the spinal cord has 33 bones which belongs to the above mentioned categories. The paper here concentrates on the Lumbar vetrebral part of the spinal cord. The lumbar vertebra has five bones between the rib cage and the pelvis, namely, a) Psoas minor (L1) b) Hip flexors (L2) c) Knee extensors (L3) d) Ankle donkiflexors (L4) e) Long toe extensors (L5). Lumbar vertebral parts are Pedicle, Articular facet, Body, Transverse process, Posterior and Anterior regions.
Medical experts have witnessed lot of spine related diseases from past two decades such as myelopathy, degenerative discs, accidental neuro vascular compilations etc. In most of these cases surgeons suggest operations. Maximum disc dislocations, accidental damages result in spine fusion surgeries. The bones which are affected the most in these damages are L4 and L5 of the Lumbar vertebra.
Implants that deal with these fusion surgeries get inserted to most intricate regions of the Lumbar vertebra where there is very less cross sectional areas; one such region is pedicle. [3] It is a small region which facilitates the screw implant fixation a strong trajectories for further support of implants, at the same time it’s intricacy makes it delicate region for screw fixation beyond which there runs a neural system from brain which in the case of misinsertion causes permanent damage and paralysis.The project here deals with automating the pedicle probe technique by configuring a robot to perform the operation with less risk of misinsertion and avoiding post operative surgical process.
Robots have had a significant impact on the manufacturing environment, yielding higher productivity and improved quality. Robots, however, have not yet made a significant impact in health care. The application of robots in medical practice is limited by a lack of tools yet to be developed. These tools are different from those in the manufacturing environment. Better visualization and control of the manipulator, as well as the opportunity for detailed pre-operative planning simulations, are of great interest to a surgeon conducting robot-assisted surgery.
In spine surgery, spinal instrumentation is often used to apply forces to correct deformity or to stabilize an injured spine. Spine instrumentation may also improve the rate and quality of biologic fusion. Spine instrumentation systems may attach to vertebrae by some combination of hooks, wires, or screws. Pedicle screw fixation is the best choice for short-segment rigid fixation or when posterior-elements are absent. One of the most critical issues to success is the exact insertion of pedicle screws. Pedicle screws may be inserted by anatomic land marks as proposed by Magerl or Camille, by extensive use of fluoroscopy which exposes both the patient and surgical team to significant radiation, by extensive dissection of the pedicle, or by some combination of these techniques. However, knowledge of the ideal positioning is one thing and accurately achieving it physically is quite another. The space where each screw can be inserted is extremely limited and is close to major vascular structures, dural tube, and nerve roots.
With the advent of robotic manipulator arms, the medical industry has endeavored to automate many procedures that require high accuracy. Total hip and knee replacements, stereotactic brain surgery, and resection of brain tumors are some of the procedures that have met with some success. In recent years, robotic technology has seen many advances that allow for accuracies of 0 0001 . " and repeatabilities 0 0005 . " .
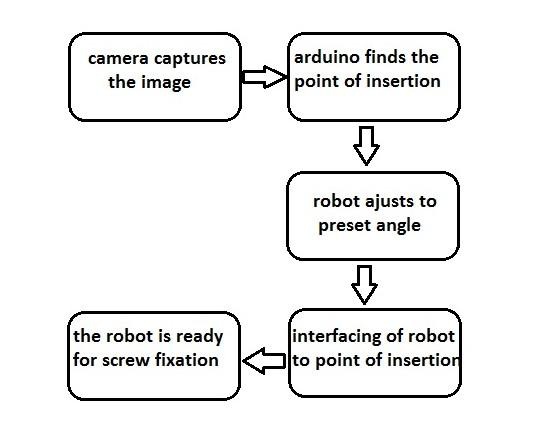
To find the point of insertion needs to be detected automatically as it is difficult for a surgeon to judge the point of insertion as he is working under blind spot.
There should be preset angular fixtures set by the robot automatically depending on the vertebrae and its standard anthropometric angular values
Automating process of pedicle screw fixation with a single robot which includes spotting the point of insertion through image processing and graphical positioning and feedback system to locate and positioning interfacing it with only robot.
The holding power of screws in bone is affected by the density to the second power, the surface area of thread-bone contact and the configuration of the thread relative to the structure of bone. Tapping of the drill hole is another source of possible loss of fixation. Frictional forces between threads and bone can have an impact on the tendency of screws to back out. It is possible to extrapolate and surmise that imprecise drill holes or tapping could compromise the stability of fixation. A concise review of screw insertion methods was presented by Goel. A recent issue of Spine was dedicated to the use of bone screws in the vertebral pedicles. A comprehensive literature review and surgical treatment alternatives as well as pedicle screw fixation mechanisms are discussed. In 1941, Lyons noted that the orthopedic literature had not addressed the subject of hole preparation for screw placement.
In this review of the current literature, it is deduced again that this issue has not been adequately addressed. Two studies were published from 1989-1991 which addressed the hole preparation technique in pedicle screw placement. Both studies compared a hand drilling technique to a hand probing technique. Pedicle screws are used for fixation in degenerative spondylolistheis, stenosis and spinal fractures. They have been found to have nearly a 20% greater rate of fusion than non-instrumented controls. There have been multiple studies reviewing pedicle screw use and complications cited have included screw loosening, pullout, migration and loss of reduction. In a recent review of 3498 cases, screw loosening was found to range from 1.7 to 2.3% depending on the indication for placement and the chronological relationship to its surgical placement (AAOl, 1994).
The anatomy of the pedicle in the thoracic and lumbar spines has been quantified for a skeletal mature population. Anatomic points on the vertebral bodies for entry into the pedicle have also been defined. Pedicle screw systems are available which should fit within the cortex of pedicles in the lower thoracic, lumbar, and sacral pedicles. Image intensification and simple radiographs have been used to guide pedicle screw placement, but radiographic assessment of pedicle screw placement has been demonstrated to show up to 8.1% false positives and up to 14.5% false negatives. Radiographically imaging the position of the screw tip relative to the anterior cortex is also difficult and misleading because of the convexity of the anterior body.
Project has the camera that captures the image of posterior part of the damaged lumbar vertebra. The image is fed to the processor and the same is displayed on the screen, the captured image undergoes edge detection technique in Matlab, which is a part of Image Processing. The edges of the lumbar vertebrae, articular facet and transverse process has coordinates through which the point of insertion is found either by drawing a straight line from the edges by dragging the cursor or by the mathematical calculations.
They can also be detected by grid techniques, machine readings etc in Matlab but the probability of getting the exact point of insertion is very less in these techniques. The point of insertion is always and must be in front of the pedicle region irrespective of the way the point is detected. The level of accuracy in finding the point of insertion is very high in edge detection technique as the coordinates read on the edges of lumbar vertebra will have exact value. The extension to this method would be automating the whole process of point detection instead of dragging.
The project is setting up a robot for particular angles. The robot is set in both transversal angle and inclination angle using servo motors for two different axes. The angle of insertion is different for different Lumbar vertebrae. All these angles are preset in the field of medicine and it is fixed on gender basis. Irrespective of size, weight and other constraints of differentiation in human body the angles of particular lumbar vertebra remains the same.
The titanium screw which has to be implanted is fixed to the robot. The extension of this part can be carried in the later stages by the image processing technique where the robot itself detects the type of the bone and automatically sets the angle by itself.The hardware components used here are Arduino UNO board, servomotor (MG995), connectors, bread board.
MATLAB
An ideal pedicle screw positioning system is one that is able to position and orient the screw such that it does not perforate anterior cortex, yet maintain a solid fusion. The depth of penetration is also important to increase pull-out strength. Placement of the screw using a manipulator is important in achieving a circular hole rather than an elliptical one resulting from manual preparation. In terms of registration, a required accuracy of ±1 mm is a goal with an orientation accuracy of two to three degrees. According to practicing orthopaedic surgeons who perform this type of fusion, a manual accuracy of 5 2 ± mm and 3 2 ± o is reported. The main problem in this type of surgery is not the accuracy of the surgeon’s hand or the manipulator’s end-effector, but is in the accuracy the data provided to the manipulator’s controller.
The extension to point of insertion method would be automating the whole process of point detection instead of dragging/grid technique.
The process of angle of insertion in the robot can be automated rather the surgeon entering the type and angles of lumbar vertebra.
Improvement in selecting a high quality servo motor.
A robot performs the operation with less risk of misinsertion and avoiding post operative surgical process.
The failure rate can definitely be reduced to less than 5% which is 20% presently.
The project will definitely be a breakthrough in the field of medicine.
The project facilitates the screw automatically into the pedicle of lumbar vertebra once the point and angle of insertion are known.
1 Bray, T.J., Templeman, D.C., Principles of screw fixation Operative Orthopaedics, 2nd Edition, J.B. Lippincott Co. Philadelphis, 1993.
2 Lyons, W.F., Cochran, J.R., Smith, L., Actuai holding power of screws in bone. Annals of Surgery, 114(3):376-384,-1941.
3 Goel, V.K., Biomechanics of the spine: Clinical and Surgical Prospective, CRC Press, Boca Raton, FL (1990).
4 Spinal Fusion: The Use of Bone Screws in the Vetrebral Pedicles, Spine, Vol. 19, No. 20S.
